


Project One:
Leveraging resident expertise on outreach
How I transformed outreach approach frameworks in East Scarborough
My Role:
I lead residents and staff through a series of co-creative design workshops and prototypes to surface pain-points, ideate, prototype, and implement innovative new approaches to outreach that became a permanently integrated framework.
The Problem:
East Scarborough is home to one of the largest populations of newcomers, non-English speakers, and vulnerable community members who are looking for accurate, trustworthy, and accessible information on community services and programs. Local service providers struggle to connect with these community members due to language barriers, lack of trust, and access.
Staff, residents, and myself set out to develop a new approach for outreach that would address language barriers, distrust, and accessibility. Within three months of exploration, creation, reflection, and implementation we designed a framework that placed residents at the forefront of outreach with staff support. The framework led to a 64% increase in referrals from the previous year, more than 90 newcomers attending a newcomer fair while remaining connected with The Storefront, and a threefold increase in residents working alongside staff.
Exploration:
Creation:
To facilitate the ideation process, I hosted co-creative workshops with local community members. In the sessions, residents observed affinity maps with the insights from the survey and focus groups which generated multiple solutions:
An outreach ambassador program where residents from each user segment would receive a small amount of compensation to conduct outreach with local residents in their network instead of staff. Staff would supply the materials and information, residents would track their conversations and attend the service/event on the day it was advertised to encourage attendance.
Local residents from each user segment to put up flyers instead of staff as they would know the best places to put the flyers to reach the residents in their networks.
Reflection:
We prototyped the two new approaches for two upcoming events: an info-session for job training opportunities in construction and a newcomer fair. Prior to the event, staff identified highly engaged local residents with relationships/networks with newcomers, non-English speakers and marginalized community members. Each resident received a contract outlining the activities they would be expected to perform as well as the number of residents they were required to engage and encourage to attend the event in exchange for an honorarium. A staff member would be responsible for checking in with residents, troubleshooting any challenges, answering questions, and supporting the residents to achieve their goals.
Implementation:
Both prototypes resulted in significant increases in awareness and attendance from the targeted user-segments. Staff were excited about the increased opportunities for engagement with residents who were new to the organization and residents felt a great sense of accomplishment and fulfillment at being able to make an impact on their communities. In order to facilitate implementation, the process was standardized and documented for all future staff and residents to replicate. Additionally, to streamline the process of getting residents their compensation a third party tool, Giftogram, was incorporated so that residents could receive their gift cards by email or in person.
What I learned:
Partnering with highly motivated residents who have the right networks can greatly improve the impact of outreach efforts.
Staff can be better utilized for creating structure and support for residents to conduct outreach.
Funders could benefit from permitting compensation structures for residents to engage in outreach work.
Project Two:
Diversity, Dialogue and Disruption
How we recentered youth perspectives and agency in youth program design frameworks
My Role:
I led a team of youth, community stakeholders and staff through a series of co-creative design workshops and prototypes to surface pain points and iterate on creative novel approaches to youth-led program design.
The Problem:
The East Scarborough community is considered to be high priority with higher rates of violence and a higher population of residents who are low income. Youth services and programming are typically designed and developed by adults. As a result, youth can feel disconnected and disengaged with the services available to them which can lead to decreased participation and retention while increasing maladaptive behavior and interactions with police.
Myself and a youth advocacy group (the Association of Committed and Engaged Youth), set out to develop a framework for new programming approaches that centered youth perspectives, needs and interests using the Service Design process of exploration, creation, reflection, and implementation. After two years of creation and implementation, we engaged 351 youth participants, increased the number of trained and active youth leaders by 500%, and were able to put together our findings and recommendations into a report that was shared with staff and stakeholders for implementation.
Creation:
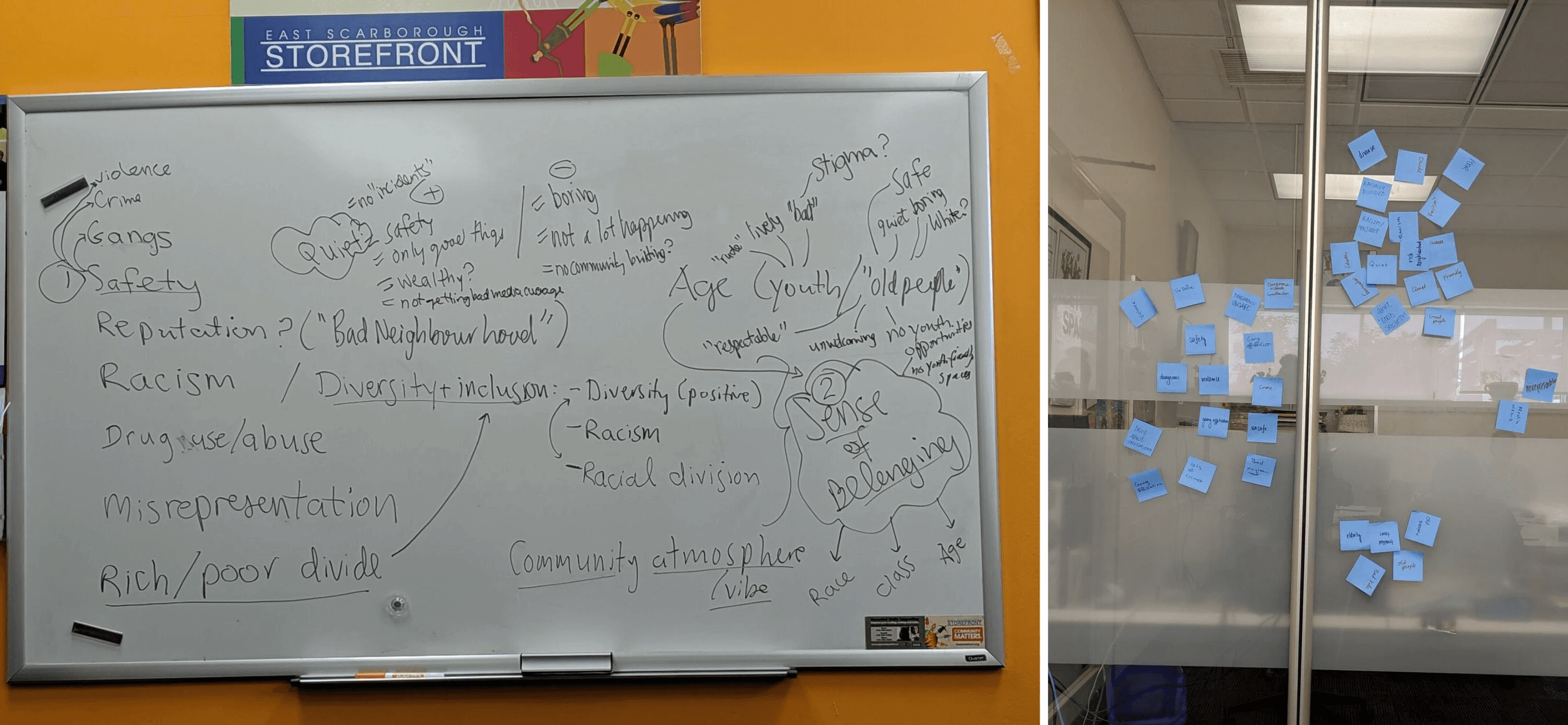
We needed to gain a better understanding of why youth feel disconnected from typical youth programming and services. However, instead of the usual approach of adults designing and asking the questions, I worked with the youth to develop questions for focus groups and surveys so that the user research would be conducted by the youth themselves. We went with this approach with the idea that increasing the level of relatability to the interviewers could improve the level of candor in interviewee responses. Whenever we could, data collection took place during co-creative sessions facilitated by the youth. In the scenario where a co-creative session could not be arranged, youth conducted surveys with students during school lunch hours. The research covered self-identity, media representation of youth, supports, and mental health resources. Demographic information was also collected.
Insights:
Youth strongly identify with their hobbies, personal interests, personality traits, and values: potentially more so than demographic characteristics such as race or age. Leveraging these hobbies and interests could help with attracting and retaining youth in programming.
When youth have the ability to represent their perspectives and experiences through media, they can counter the negative stereotypes and perceptions that they internalize from dominant media narratives.
Increased communication and integration between youth supports offered within schools and the wider community would increase the level of accessibility, accommodation and peer-led options for youth.
Mental health resources can only be effective if youth are both aware of their existence and are willing to use them. As mentioned in previous insights, increasing the level of integration that community mental health resources have with schools would increase awareness with youth, while leveraging their personal interests would increase participation.
Reflection:
The co-creative sessions also served as opportunities to prototype the youth-centered approach as we gathered insights in real time. Here's how:
The research questions were designed and administered by youth ensuring that youth perspectives and experiences were centered.
Youth facilitators leveraged the hobbies, interests, and personality traits during workshop activities to encourage more in depth and productive discussions.
At every co-creative session, youth were given a presentation on some of the youth supports and mental health resources in the community available to them. They were also provided with a more exhaustive list to take home with the intention of increasing their awareness and willingness to utilize them.
Adults did not actively participate in the workshops, they either observed or assisted where necessary.
We were unable to work on increasing the level of communication and integration of wider reaching community support and resources in schools due to time constraints and COVID-19 lockdown measures.
The insights gathered from the co-creative sessions resulted in a rich report that was shared with stakeholders, funders, youth, and Storefront staff. We received positive feedback on the sessions from all the players including teachers and youth workers. The youth facilitators gained a lot of confidence and essential data to back up their youth-advocacy work. In fact, the report was instrumental to both the East Scarborough Storefront (ESS) and the Association of Committed and Engaged Youth (ACEY) during the Ontario lockdown measures that began on March 17, 2020.
Implementation:
While most youth serving institutions and organizations either completely shut down operations or had challenges transitioning to online, ESS with the support of ACEY was able to quickly pivot youth programming from in person to digital. Knowing that youth were already gathering on platforms like Discord, ACEY leveraged their interests in gaming, art, and media to create a digital space in place of a physical one. The online sessions were hosted by youth facilitators from ACEY instead of adults to ensure youth perspectives and experiences were represented. The purpose of these sessions were to support youth mental health during lockdown so each session included resources and activities from local community organizations and supports. Without established integrations and communication with wider community organizations, we were unable to implement the framework in schools as they transitioned to online. All of the sessions were well attended with highly active participants.
What I learned:
A youth centered framework can mitigate against service disruptions due to crises such as pandemics. The approach allows for the ability to adapt to rapidly changing contexts where youth may not be able to gather together in person to access services.
Stronger relationships between youth serving institutions and community wide resources/services are necessary for youth to be aware of and access resources and services but establishing and maintaining these relationships requires additional time, funding and buy-in from all players involved.
Project Three:
Hi Henrietta
How we leveraged AI to improve health outcomes and experiences for Black patients in Canada
My Role:
Myself and another designer conducted user research, data synthesization, wireframing, prototyping and user testing.
The Problem:
Black patients in Canada have negative experiences navigating the Canadian health care system due to a shortage of culturally sensitive health care providers which leads to long wait times, delayed or no care, late or misdiagnosis and worse health outcomes.
I worked with a cross-functional team to run design sprints over 8 weeks using design thinking principles and methodologies that included empathizing, defining the problem, ideation, prototyping, and testing. After iterating we were able to design a prototype of a web-responsive health chatbot application that utilizes AI to support the personalized and culturally sensitive diagnosis and triaging of Black patients to improve their experience with the Canadian health care system. We acquired 46 newsletter sign-ups for product updates in one week and our team placed second in a product pitch competition.
Empathize:
Initially the team hypothesized that Black patients needed tools to support self-advocacy, specifically an application to help them understand medical language so that they could better discuss their symptoms with medical professionals, improving communication and potentially speeding up access to accurate diagnosis and potentially improving health outcomes.
To test our hypothesis, I collaborated with another product designer to develop 16 questions for user interviews to hear the experiences of Black patients navigating the Canadian health care system, in-depth. I also collaborated with the business analysts to develop a 15 question survey so that we could gather qualitative and quantitative data from a wide audience. The business analysts also conducted competitive analysis so that we could surface opportunities for improvement over competitor applications.
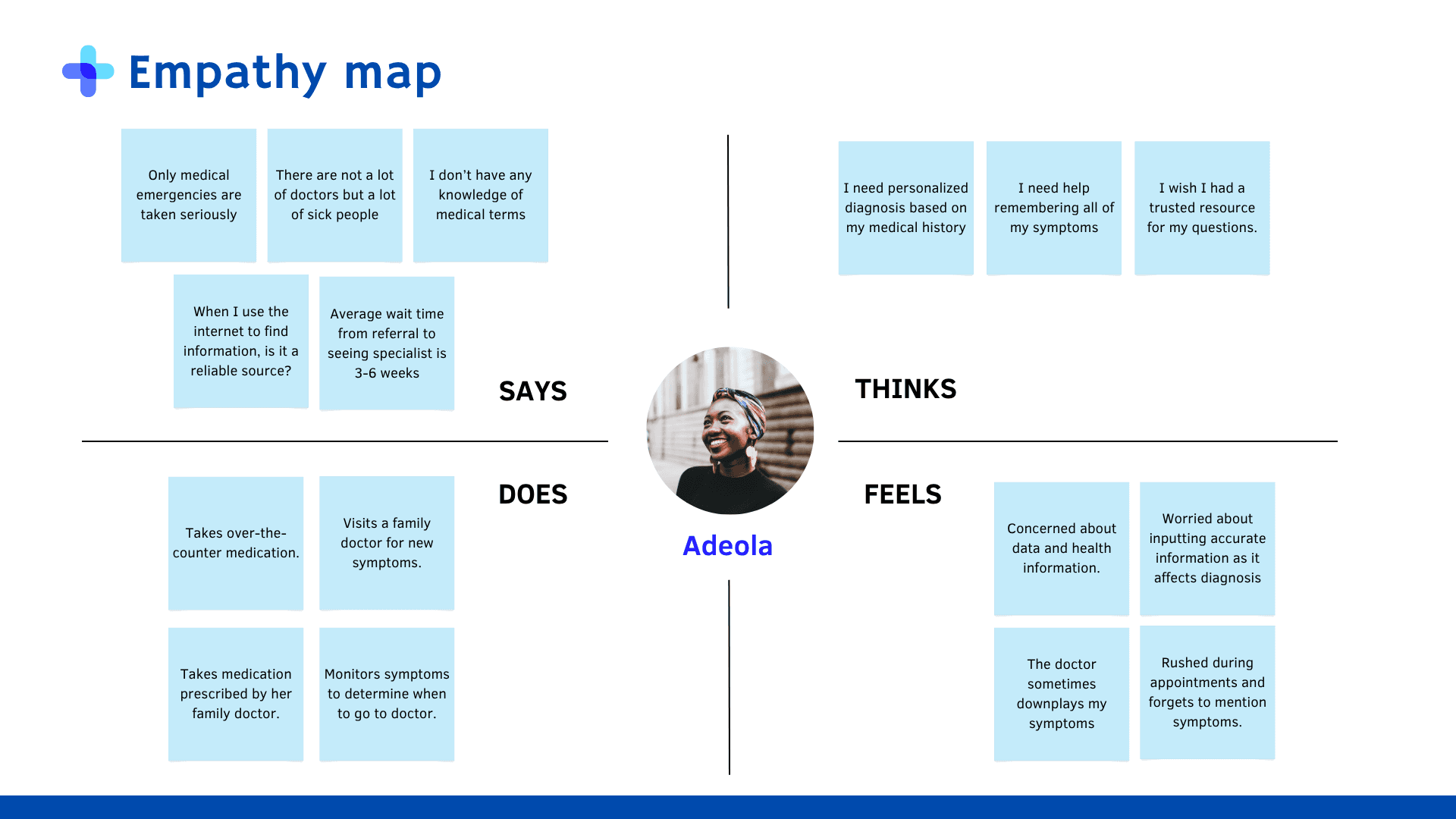
We conducted nine user interviews and received 40 responses to the survey. Myself and another designer synthesized the data using empathy maps to develop a user personas which enabled us to narrow scope on the core features and functionality of the application.
Insights:
The data revealed the following pain points for users:
Delays in access: When Black patients do seek healthcare they experience increasingly long wait times to access a doctor and even longer wait times for accessing specialists for follow-up.
Symptom minimization or dismissal: When Black patients are able to engage with medical professionals they feel the appointments are rushed and that the doctors do not take their symptoms seriously, missing opportunities for referrals or accurate diagnosis.
Lack of personalization: When Black patients attempt to resolve healthcare matters on their own via seeking answers online, the results often lack consideration for their personal medical history and additional factors such as race or culture.
These insights shifted our focus from supporting patients with self-advocacy to supporting medical professionals and patients with triage and diagnosis. In our design concept, users would need a way to input their medical and demographic information for personalization. Users would also need a way to input their symptoms and receive potential diagnosis from a database with reliable and trustworthy information to reduce symptom minimization or dismissal. Based on the symptoms they input, they would also need advice on whether or not to access medical care, reducing delays in access by sifting out patients who seek medical care unnecessarily.
Define:
Using the insights we gathered, I mapped key service touchpoints using a user journey map of the current user experience. The user journey map provided a useful visual aid for facilitating a session with my cross-functional team to define the problems for our users and surfacing opportunities for solutions.
User Journey Map (Current)
Prototype:
While my fellow designer and I collaborated throughout the entire design process, we delegated user flows to increase productivity and efficiency. I was responsible for the profile creation (which includes medical history input and demographics input), and symptom analysis user flows.
Profile creation, medical history and demographic information
Ideally, our team would partner with medical institutions and agencies to auto populate patient history and information. However, in the case where a patient cannot access the healthcare system, they should have the option to enter or update their information manually.
Initially I designed and organized the medical history frames to be similar to a patient intake form as this would be familiar to most users who have engaged with the healthcare system. However, this approach would have made the process too long and laborious for users, especially if they are using the app on smaller devices like their phones.
How I Adapted and Iterated
To address these challenges, I iterated on the design to reduce the number of screens required and reduced the amount of effort required to input information.
Wireframe
Mockup
Click to enlarge the image.
Symptom Analysis
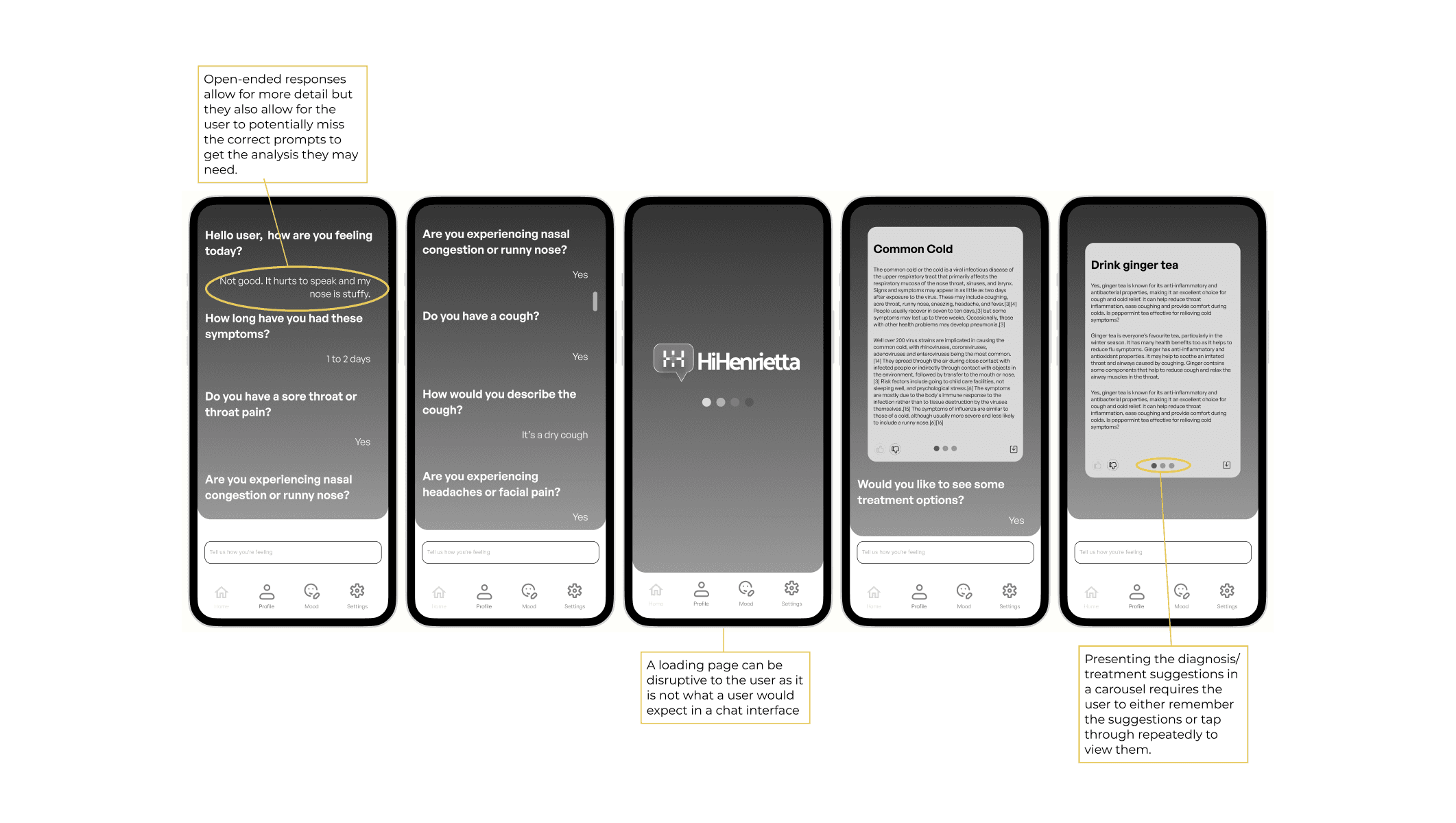
The core feature of the application is to provide users with a way to discuss their symptoms with a chatbot who can process their inputs and make recommendations about their potential diagnoses and treatment options by referencing medical databases.
Originally, I prioritized users having the ability to express themselves in detail regarding their symptoms and viewing the detailed description of one diagnosis/treatment suggestion prior to seeing the rest. However, I received feedback from the developers that users may not input the correct prompts required to get the most accurate and usable responses from the chatbot. Additionally, a user needing to tap through a carousel to see the diagnosis/treatment suggestions increases their mental load as they either have to memorize the suggestions or tap through to review the suggestions again.
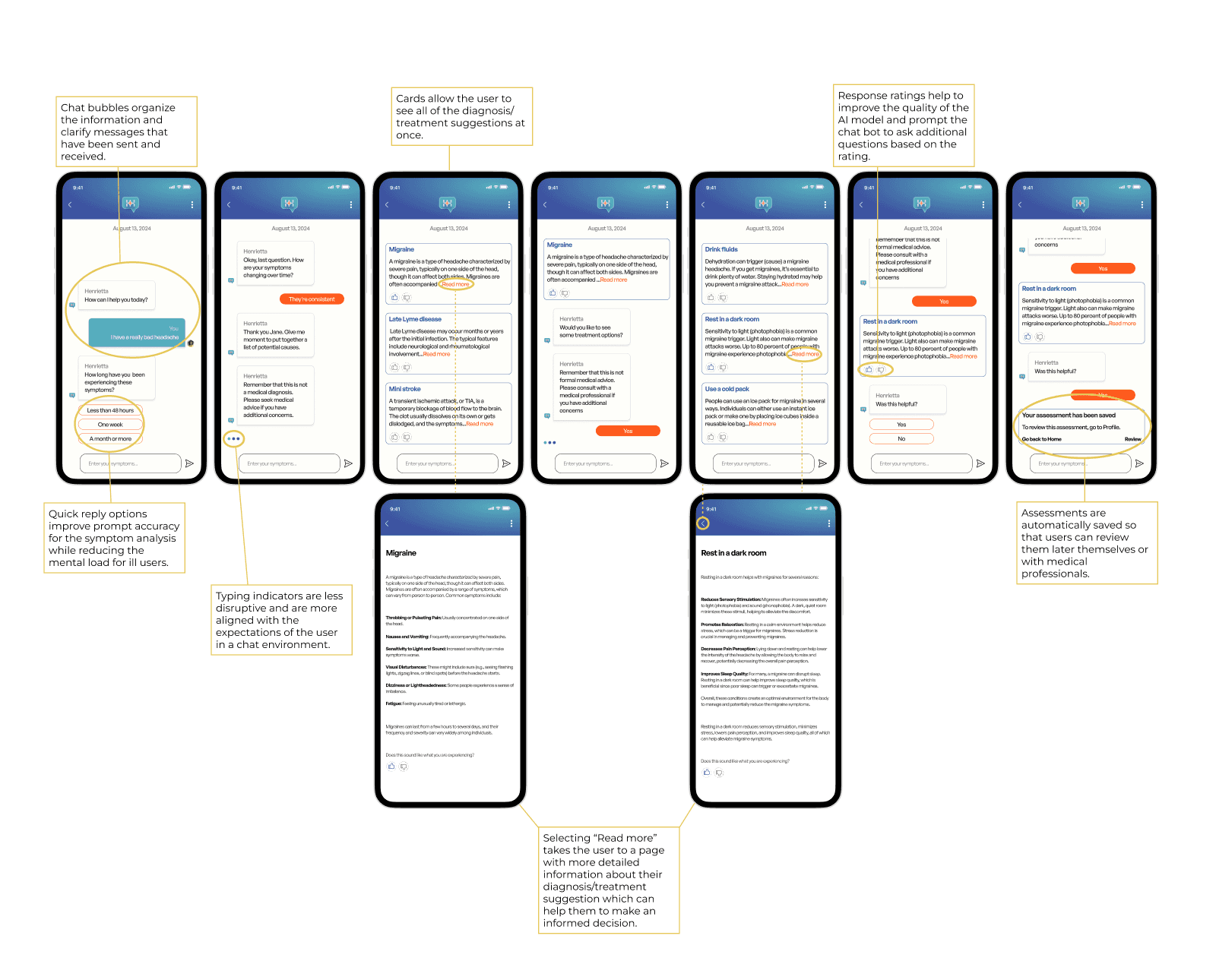
How I Adapted and Iterated
To address this feedback, I researched to learn more about how prompt engineering works and changed the design to include a list of prompts from which users could select to respond to the chatbot. The change had an added benefit of reducing the amount of mental load required of the potentially ill user to answer the questions of the chatbot. To correct this, I changed the UI so that all options would be presented at once, if users want to read the detailed descriptions of each diagnosis/treatment suggestion they can select the "read more" link which redirects them to a page with a longer description.
Wireframe
Mockup
Click to enlarge the image.
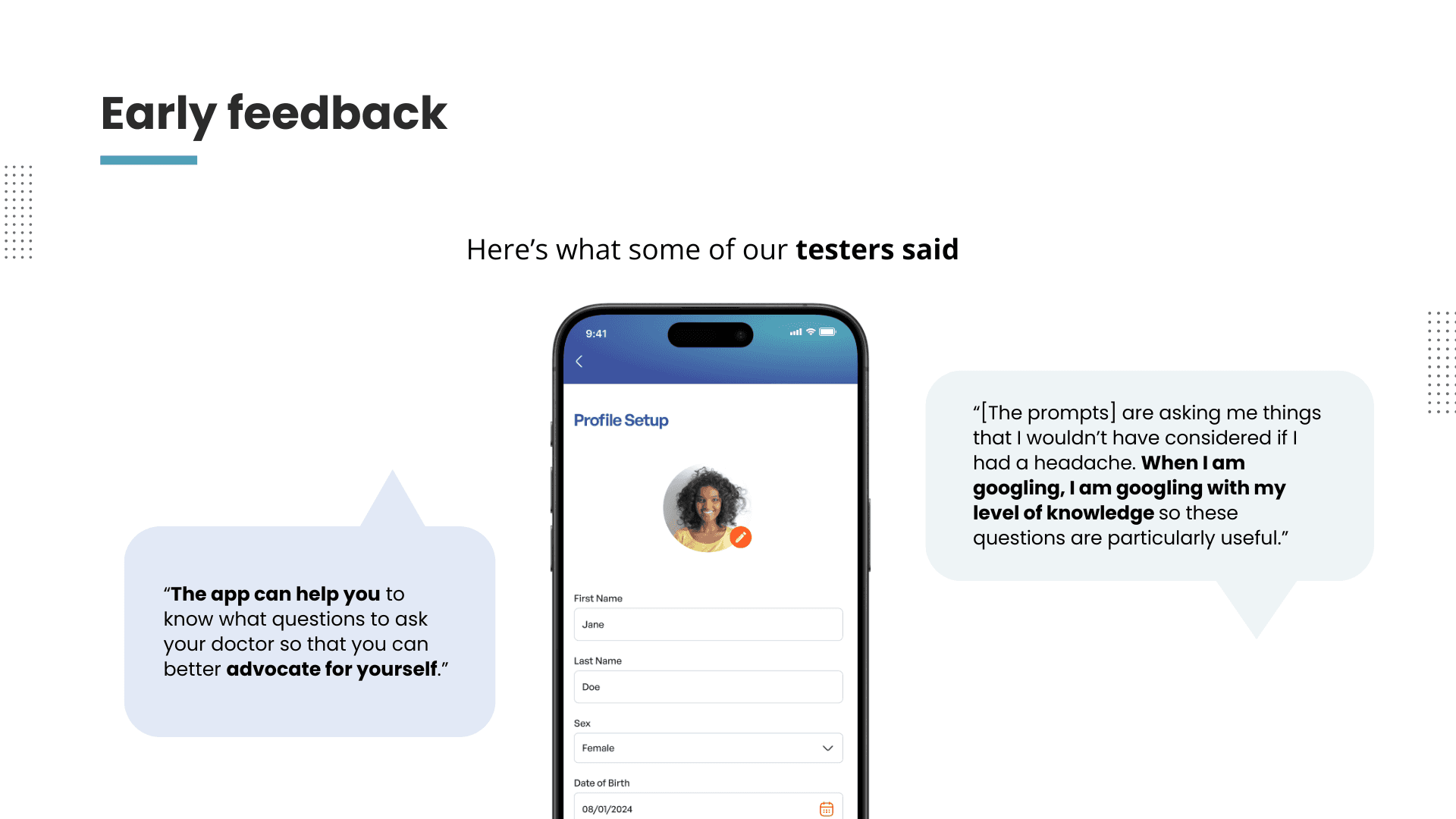
We received very positive feedback from the usability tests we conducted on our finalized prototype. Users appreciated the way the medical history and demographic input pages were organized as they felt that there was a lot of thought put into how and why the information was being collected. They also appreciated the way that the chatbot asked questions that they would not have considered on their own when attempting self-diagnosis. In terms of improvement, we received feedback that the amount of information we provided in both the diagnosis and treatment suggestions were overwhelming, so we shortened them in the final prototype.
What I learned:
Designing for AI requires understanding how both humans and AI generators “think” in order to best get the results that users want.
Users are still looking for human-like experiences even when they are interacting with AI. This is especially the case with Black patients navigating the health care system where they already feel dehumanized at times.